
Cheat wall deformity
Introduction
Chest
wall: The
thoracic wall or chest wall is the boundary of the thoracic cavity. The bony
portion is known as the thoracic cage. However the wall also includes muscles,
Skin & fascia.
Chest
wall deformity:
Chest wall deformities are fairly common structural deformity in the chest
wall.
Types: There are two basic kinds of
chest wall deformity:
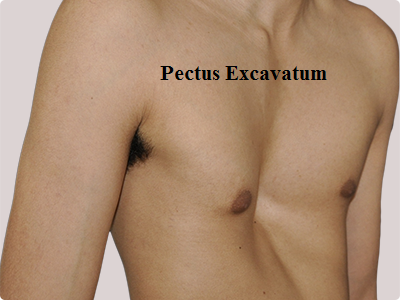
1. Pectus excavatum
2. Pectus carinatum
Pectus excavatum
Definition
Pectus excavatum is a condition in
which a person's breastbone is sunken into his or her chest. The chest bows
inward instead of outward. In severe cases, pectus excavatum can look as if the
center of the chest has been scooped out, leaving a deep dent.
While the sunken breastbone is often
noticeable shortly after birth, the severity of pectus excavatum typically
worsens during the adolescent growth spurt.
Also called funnel chest, pectus
excavatum is more common in boys than in girls. Severe cases of pectus
excavatum can eventually interfere with the function of the heart and lungs.
But even mild cases of pectus excavatum can make children feel self-conscious
about their appearance. Surgery can correct the deformity.
·
Also
known as sunken or funnel chest. It is the most congenital abnormality of the
chest wall.
·
When
the bone caves into the chest forming a depression or cup like structure is
called pectus excavatum. It occurs in 1 out of 500 children and occurs mostly
in girls.
Pathophysiology
Because
the heart is located behind the sternum, and because individuals with pectus
excavatum have been shown to have visible deformities of the heart (seen both
on radiological imaging and after autopsies), it has been hypothesized that
there is impairment of function of the cardiovascular system in individuals
with pectus excavatum. While some studies have demonstrated decreased
cardiovascular function in pectus excavatum, there has been no consensus
reached based on newer physiological tests (such as echocardiography) of the presence or degree of
impairment in cardiovascular function in people with pectus excavatum.
Similarly, there is no consensus on the degree of functional improvement after
corrective surgery.
Symptoms
For many people with pectus
excavatum, their only sign or symptom is a slight indentation in their chests.
In some people, the depth of the indentation worsens in early adolescence and
can continue to worsen into adulthood.
In severe cases of pectus excavatum,
the breastbone may compress the lungs and heart. Signs and symptoms may
include:
- Decreased
exercise tolerance
- Rapid
heartbeat or heart palpitations
- Recurrent
respiratory infections
- Wheezing
or coughing
- Chest
pain
- Heart
murmur
- Fatigue
Causes
While the exact cause of pectus
excavatum is unknown, it may be an inherited condition because it sometimes
runs in families.
Pectus excavatum can occur in
conjunction with other medical conditions, such as:
- Marfan
syndrome. This hereditary condition
affects the connective tissue, often resulting in limbs and fingers that
are especially long and thin.
- Scoliosis.
An abnormal curvature of the spine, scoliosis usually occurs in
pre-adolescent girls.
- Mitral
valve prolapse. The mitral valve separates the
two chambers of the left side of the heart. Defects in the mitral valve
may reduce the heart's efficiency in pumping blood.
Risk factors
Pectus
excavatum is more common in boys than in girls.
Complications
Multimedia
Severe cases of pectus excavatum can
compress the lungs and push the heart over to one side. Even mild cases of
pectus excavatum can result in self-image problems.
Heart and lung problems
If the depth of the breastbone
indentation is severe, it may reduce the amount of room the lungs have to
expand. This compression can also squeeze the heart, pushing it into the left
side of the chest and reducing its ability to pump efficiently.
Self-image problems
Children who have pectus excavatum
also tend to have a hunched-forward posture, with flared ribs and shoulder
blades. Many are so self-conscious about their appearance that they avoid
activities, such as swimming, where the indentation in their chests is more
difficult to camouflage with clothing
Tests and diagnosis
Pectus excavatum can usually be
diagnosed simply by examining the chest. But your doctor may suggest several
different types of tests to check for associated problems with the heart and
lungs. These tests may include:
- Chest
X-ray. This test can visualize the
dip in the breastbone and often shows the heart being displaced into the
left side of the chest. X-rays are painless and take only a few minutes to
complete.
- Computerized
tomography (CT). A CT scan may be used to help
determine the severity of the pectus excavatum and whether the heart or
lungs are being compressed. CT scans take many X-rays from a variety of
angles to produce cross-sectional images of the body's internal structure.
- Electrocardiogram.
An electrocardiogram can show whether the heart's rhythm is normal or
irregular, and if the electrical signals that control the heartbeat are
timed properly. This test is painless and involves the placement of more
than a dozen electrical leads, which are attached to the body with a
sticky adhesive.
- Echocardiogram.
An echocardiogram is a sonogram of the heart. It can show real-time images
of how well the heart and its valves are working. The images are produced
by transmitting sound waves via a wand pressed against the chest.
- Lung
function tests. These types of tests measure
the amount of air your lungs can hold and how quickly you can empty your
lungs. In some cases, these tests are performed while the person is
exercising on a treadmill.
- Exercise
test. This test monitors how well
your heart and lungs function while you exercise, usually on a treadmill.
Treatments and drugs
Pectus excavatum can be surgically
repaired, but surgery is usually reserved for people who have moderate to
severe signs and symptoms. People who have mild signs and symptoms may be
helped by physical therapy. Certain exercises can improve posture and increase
the degree to which the chest can expand.
If you have mild pectus excavatum,
your doctor may want to re-evaluate you every six to 24 months, to make sure
your symptoms haven't worsened.
Types of surgery
If you have moderate to severe
pectus excavatum, your doctor may suggest surgery. The two most common types of
surgeries used to correct pectus excavatum differ by the size of the incisions
used:
- Larger
incision. The larger,
center-of-the-chest incision used in the Ravitch technique allows the
surgeon to view the breastbone directly. The abnormal cartilage attaching
the ribs to the lower breastbone is removed and the breastbone is fixed
into a more normal position with surgical hardware, such as a metal strut
or mesh supports. These supports are removed in nine to 12 months.
- Smaller
incisions. In the minimally invasive Nuss
procedure, small incisions are placed on each side of the chest, under
each arm. Long-handled tools and a narrow fiber-optic camera are inserted
through the incisions. A curved metal bar is threaded under the depressed
breastbone, to raise it into a more normal position. In some cases, more
than one bar is used. The bars are removed after two years.
Comparable risks and outcomes
Both the Ravitch and Nuss procedures
have been revised and improved over the years. While the Ravitch technique
takes longer to complete, the Nuss procedure typically results in a longer
hospital stay. Success rates are higher at hospitals that perform more of these
types of surgeries.
Most people who undergo surgery to
correct pectus excavatum are happy with the change in how their chests look, no
matter which procedure is used. Either procedure also improves heart function.
Best results are achieved when the surgery is performed after the age of 8 and
before the end of adolescence, but adults also have benefitted from these types
of surgeries.
Pectus Carinatum
Pectus
carinatum, (L
carīnātus, equiv. to carīn(a) keel), also called pigeon chest, is a
deformity of the chest characterized by a protrusion of the sternum and ribs.
It is the opposite of pectus excavatum.
It
also known as pigeon chest. When the bone pushes outward forming a moud like
structure characterized by protution of sternum & ribs. Occurs in 1 out of
1500 children and occure mostly in boys.

Can
cause scoliosis. It is the opposite of pectus excavatum.
Pathogenesis:
No specific cause is
identified but there is an association with other skeletal abnormalities. Such
as scoliosis suggesting that connective tissue disease in some cases may play a
role in its pathogenesis.
Common Causes
- Congenital
pectus carinatum (present at birth)
- Trisomy 18
- Trisomy
21
- Homocystinuria
- Marfan syndrome
- Morquio
syndrome
- Multiple
lentigines syndrome
- Osteogenesis
imperfecta
Clinical
presentation:
1.
May patient with this defect area.
Asumptomatic.
2.
Patient with severe anomalies may
complain of pain wher lying in the prone position.
Epidemiology
Pectus deformities are common; about 1 in 400
people have a pectus disorder.
Pectus carinatum is rarer than pectus
excavatum, another pectus disorder, occurring in only about 20% of people
with pectus deformities. About four out of five patients are males.
Symptoms
People
with pectus carinatum usually develop normal hearts and lungs, but the
deformity may prevent these from functioning optimally. In moderate to severe
cases of pectus carinatum, the chest wall is rigidly held in an outward
position. Thus, respirations are inefficient and the individual needs to use
the accessory muscles for respiration, rather than normal chest muscles, during
strenuous exercise. This negatively affects gas exchange and causes a decrease
in stamina. Children with pectus deformities often tire sooner than their
peers, due to shortness of breath and fatigue. Commonly concurrent is mild to
moderate asthma.
Some
children with pectus carinatum also have scoliosis (curvature of the spine). Some have mitral
valve prolapse, a
condition in which the heart mitral valve functions abnormally. Connective
tissue disorders involving structural abnormalities of the major blood vessels
and heart valves are also seen. Although rarely seen, some children have other
connective tissue disorders, including arthritis, visual impairment and healing
impairment.
Apart
from the possible physiologic consequences, pectus deformities can have a
significant psychologic impact. Some people, especially those with milder
cases, live happily with pectus carinatum. For others, though, the shape of the
chest can damage their self-image and confidence, possibly disrupting social
connections and causing them to feel uncomfortable throughout adolescence and
adulthood. As the child grows older, especially if male, bodybuilding
techniques may be useful for balancing visual impact.
Prognosis
Pectus
deformities usually become more severe during adolescent growth years and may
worsen throughout adult life. The secondary effects, such as scoliosis and
cardiovascular and pulmonary conditions, may worsen with advancing age.
Body
building exercises (often attempted to cover the defect with pectoral muscles)
will not alter the ribs and cartilage of the chest wall, and are generally
considered not harmful.
Most
insurance companies no longer consider chest wall deformities like pectus
carinatum to be purely cosmetic conditions. While the psychologic impact of any
deformity is real and must be addressed, the physiological concerns must take
precedence. The possibility of lifelong cardiopulmonary difficulties is serious
enough to warrant a visit to a thoracic surgeon.
Treatment
External bracing technique
In
children, teenagers, and young adults who have pectus carinatum and are
motivated to avoid surgery, the use of a customized chest-wall brace that
applies direct pressure on the protruding area of the chest produces excellent
outcomes. Willingness to wear the brace as required is essential for the
success of this treatment approach. The brace works in much the same way as orthodontics (braces that correct the alignment
of teeth). The brace consists of front and back compression plates that are
anchored to aluminum bars. These bars are bound together by a tightening
mechanism which varies from brace to brace. This device is easily hidden under
clothing and must be worn from 14 to 24 hours a day. The wearing time varies
with each brace manufacturer and the managing physicians protocol, which could
be based on the severity of the carinatum deformity (mild moderate severe) and
if it is symmetric or asymmetric.
Depending
on the manufacturer and/or the patient's preference, the brace may be worn on
the skin or it may be worn over a body 'sock' or sleeve called a Bracemate,
specifically designed to be worn under braces. A physician or orthotist or
brace manufacturer's representative can show how to check to see if the brace
is in correct position on the chest.
Bracing
is becoming more popular over surgery for pectus carinatum, mostly because it
eliminates the risks that accompany surgery. The prescribing of bracing as a
treatment for pectus carinatum has 'trickled down' from both paediatric and
thoracic surgeons to the family physician and pediatricians again due to its
lower risks and well-documented very high success results.
Regular
supervision during the bracing period is required for optimal results.
Adjustments may be needed to the brace as the child grows and the pectus
improves.
If
the person with PC is not treated with a brace by the end of puberty, the brace
technique is not an option, as the shape of the ribcage and sternum are set for
the rest of their lives.
Surgical
For
patients with severe pectus carinatum, surgery may be necessary. However
bracing could and may still be the first line of treatment. Some severe cases
treated with bracing may result in just enough improvement that patient is
happy with the outcome and may not want surgery afterwards.
If
bracing should fail for whatever reason then surgery would be the next step.
The two most common procedures are the Ravitch technique and the Reverse Nuss procedure.
The
Nuss was developed by Donald Nuss at the Children's Hospital of the King's
Daughters in Norfolk, Va. The Nuss is primarily used for Pectus Excavatum, but
has recently been revised for use in some cases of PC, primarily when the
deformity is symmetrical.
Other options
After
adolescence, some men and women use bodybuilding as a means to hide their
deformity. Some women find that their breasts, if large enough, serve the same
purpose. Some plastic surgeons perform breast augmentation to disguise mild to
moderate cases in women. Bodybuilding is suggested for people with symmetrical
pectus carinatum.
মন্তব্যসমূহ
একটি মন্তব্য পোস্ট করুন