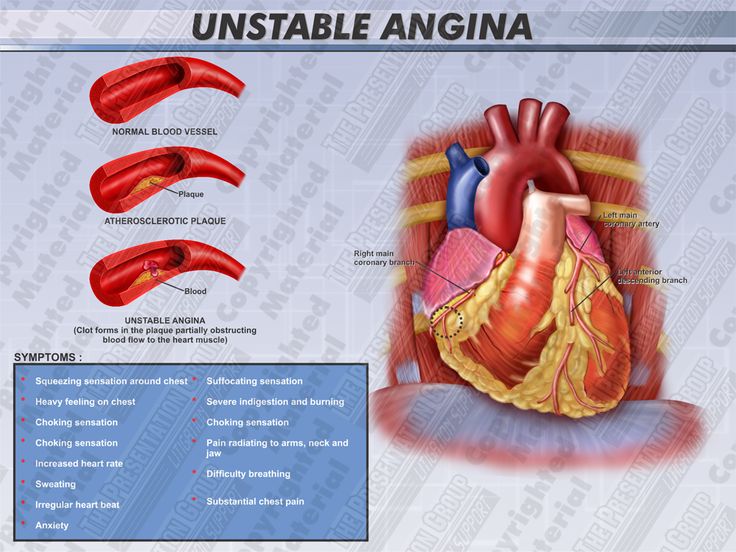
Unstable by angina is a
clinical syndrome that is characterized by new-onset or rapidly worsening
angina (Crescendo angina), angina on minimal exertion or angina at rest in the
absence of myocardial damage.
Acute coronary syndrome
is a term that encompasses both unstable angina and myocardial infarction.
Pathogenesis:
Fissuring of atheromatous plaque which is associated with thrombosis or
vasospasm (supply led ischemia).In contrast stable angina is related to a fixed
obstruction and usually precipitated by an increase in myocardial oxygen
demand.
ECG:
In patient with unstable angina or partial thickness myocardial infarction the
ECG shows ST/T wave changes and T wave inversion; the T wave changes are
sometimes prolonged.
Characteristics:
·
More severs.
·
More frequent ( 3 or more attacks per
day)
·
More prolonged.
·
Provoked by less exertion or even at
rest.
·
Less relived by usual remedial measure.
·
Referred to new sites.
·
Unusual new symptoms.
Unstable
angina: Risk stratification:
High
risk
|
Low
risk
|
|
Clinical
|
Post
infraction angina. Recurrent pain at rest. Heart failure.
|
No
history of MI. Rapid resolution of symptoms.
|
ECG
|
Arrhythmia.
ST
depression.
Transient
ST elevation.
Persistent
deep T wave inversion.
|
Minor
or no ECG changes.
|
Biochemistry
|
Troponin
T >0.1 µg/L
|
Troponin
T < 0.1µg/L
|
Management:
[A]
Initial treatment:
a)
Immediate hospitalization.
b)
Bed rest.
c)
Aspirin: 300 mg followed by 75-325 mg
daily long term and clopidogrel 300 mg followed by 75 mg daily for 12 months.
d)
Β-blocker: Atenolol 50-100 mg daily or
metoprolol 50-100 mg 12 hourly.
e)
Calcium channel blocker: Nifedipine
(with β blocker).
f)
Anticoagulant therapy with heparin (i/v
infusion of unfractional heparin with does adjusted thrombin time, or as
subcutaneous low molecular wt. heparin)
[B]
If pain persists or recurs: Intravenous nitrates- GTN 0.6-1.2
mg/hour or isosorbide dinitrate 1-2 mg/hour.
[C]
If medical treatment fails: Emergency coronary angiography
should be done then PTCA or CABG.
Reference:
1. Davidson’s Principle and Practice
of Medicine, 21st edition.
2. Wikipedia the free encyclopedia.
মন্তব্যসমূহ
একটি মন্তব্য পোস্ট করুন